

Why portacath?
A portacath is an implanted venous access device for patients who need frequent or continuous administration of chemotherapy or other long term intravenous therapy. Drugs used for chemotherapy are often irritant to the skin and veins. Therefore, they often need to be delivered into large central vein where the drugs are immediately diluted by the blood stream and delivered efficiently to the entire body. Ports may also be used for withdrawing blood for tests and certain modern ports can also be used as access for intravenous contrast administration for imaging tests such as CT scans. Using minimally invasive image-guided techniques, the portacaths that are implanted are highly appreciated by patients, oncology nurses and doctors. The procedure is easily performed with minimal risk and discomfort.
What is a portacath?
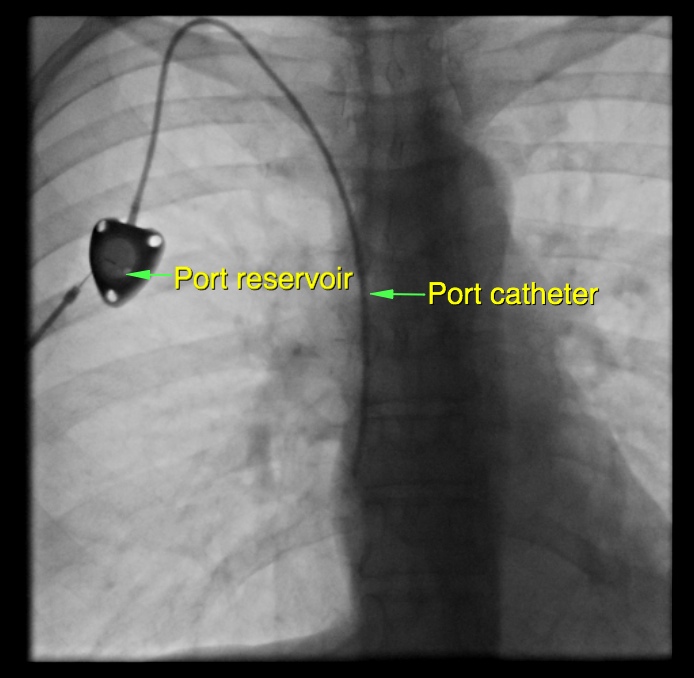 A portacath consists of a reservoir (the portal) and a tube (the catheter). The reservoir is implanted pocket formed under the skin in the upper chest. The catheter runs in a tunnel under the skin, enters a large vein just above the collar bone and is advanced to the largest vein in the body, adjacent to the heart. Since it is completely internal, it is not visible externally and is sequestered from the external environment when not in use. The septum of the portal is made of a special self-sealing silicone rubber. It can be punctured up to hundreds of times and therefore can be used for many years if required.
A portacath consists of a reservoir (the portal) and a tube (the catheter). The reservoir is implanted pocket formed under the skin in the upper chest. The catheter runs in a tunnel under the skin, enters a large vein just above the collar bone and is advanced to the largest vein in the body, adjacent to the heart. Since it is completely internal, it is not visible externally and is sequestered from the external environment when not in use. The septum of the portal is made of a special self-sealing silicone rubber. It can be punctured up to hundreds of times and therefore can be used for many years if required.
How is a portacath used?
The port can be palpated with the fingers. Prior to usage, the skin over the port is sterilized. The port is accessed by puncturing through the overlying skin with a Huber needle. The needle is specially designed so that it will not damage the silicone septum. After each use, the port is flushed with saline followed by dilute heparin to prevent clotting.
How is a portacath implanted?
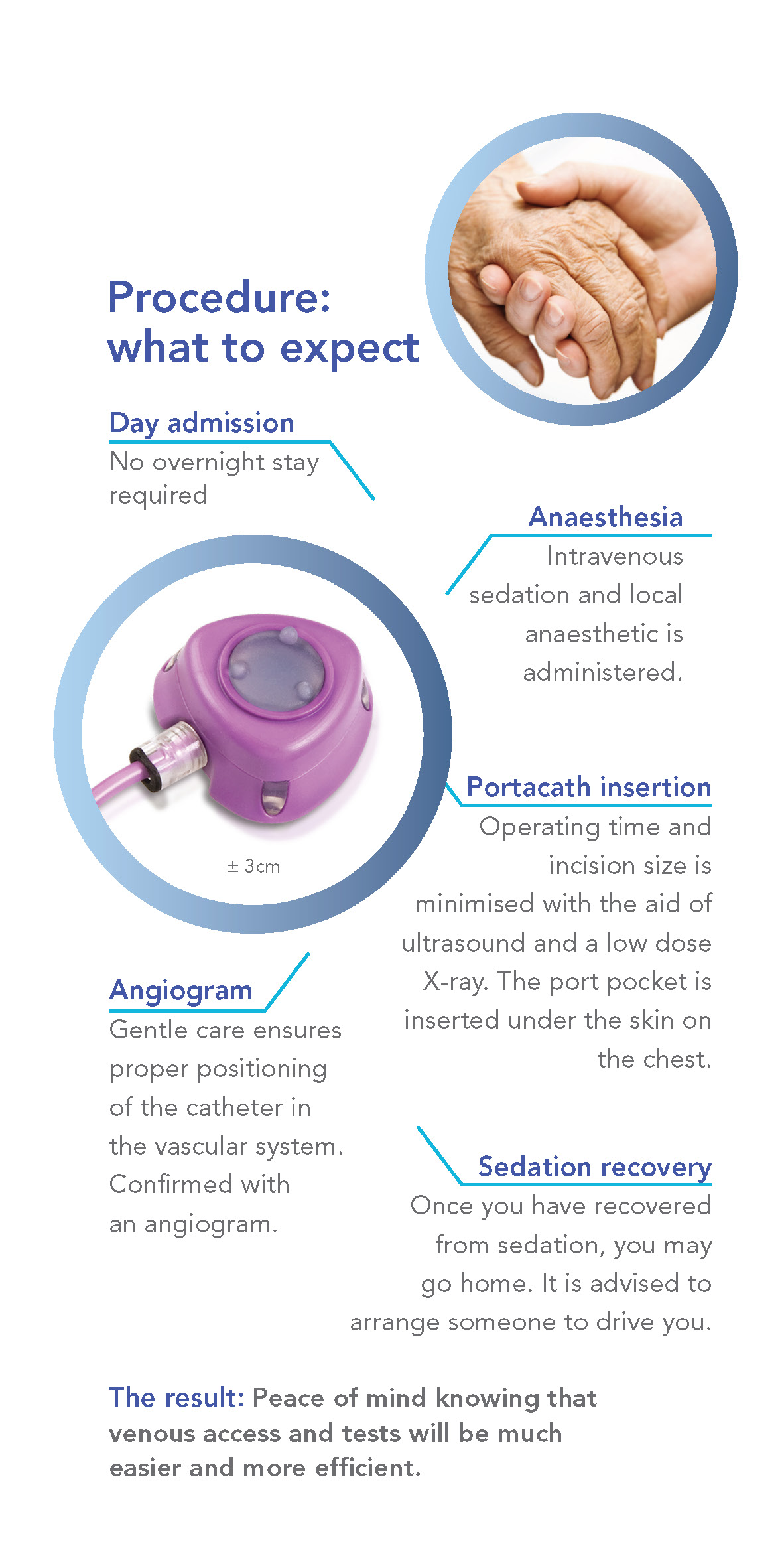
The procedure is performed with the aid of imaging guidance (ultrasound and X-ray) in the angiography suite. Care is taken to ensure proper positioning of the catheter in the vascular system and this is confirmed with an angiogram. The actual procedure takes less than an hour and is performed under intravenous sedation. There will be a small skin incision on the chest wall for the port pocket and a tiny incision in the lower neck to enter the vein. Absorbable sutures are used for the chest wound and these are buried under the skin.
You may go home two hours following the procedure, when you have recovered from the sedation.
What preparation is required?
You need to avoid solid food from midnight prior to the procedure. Clear fluid and medications are allowed up to the time of procedure. If you are on blood thinning agents such as aspirin, warfarin or plavix, please consult with your doctor prior to the procedure.
What after-care is required?
For 7 days after the procedure, the wound should be kept clean and dry. Use a hand held shower-head to avoid getting the wound wet, otherwise sponge or bathe instead. Avoid strenuous activities of the upper limb and chest wall, to optimize wound healing. The dressing can be removed after 7 days. When portacaths are not regularly used, they need to be flushed with saline and locked with heparinised saline once per month to remain patent. If the portacath is no longer required, we can remove it. The procedure is performed under sedation and local anaesthetic, similar to insertion.
Why are portacaths implanted by Interventional Radiologists?
Our Interventional Radiologists are sub-specialists in using state of the art imaging in order to perform minimally invasive procedures. The actual puncture is performed under real-time ultrasound guidance, thus avoiding injury to the adjacent artery. Once the vein is punctured, a guide wire is inserted and its position is checked with X-ray. The length of catheter required is measured with X-ray. Finally the function of the portacath is checked by injection of X-ray dye.
What are the risks of portacath insertion?
With modern imaging guidance, the risk of the procedure itself is extremely low. There are theoretical risks of blood vessel injury, wound infection, bruising and haematoma formation, and the very remote chance of allergic reaction to the X-ray dye and drugs used during the procedure.